Abstract
Mucoceles are gradually expanding lesion involving paranasal sinuses. This is usually caused due to obstruction to the normal drainage channels of paranasal sinuses leading on to pent up secretions within it. These patients classically don’t present with symptoms pertaining to nose and sinuses but with ophthalmological signs and symptoms. They invariably present to the opthalmologist before finding their way to an otolaryngologist.
Mucoceles of paranasal sinuses
Definition:
A mucocele is defined as mucous filled epithelium lined sac. Mucoceles commonly involve ethmoidal and frontal sinuses. Mucoceles are commonly caused due to obstruction to drainage channel of paranasal sinuses. These expansile cystic masses are sometimes filled with mucopurulent secretions 1. Sometimes associated bone destruction is also evident 2.
Mucoceles are rather common in frontal sinuses. Next comes the ethmoidal sinuses. Isolated mucoceles involving ethmoidal sinuses are rather rare 5. They always occur in combination with frontal / sphenoid mucoceles 4.
History:
The term mucocele was first coined by Rollet in 1896. Onodi first described histology of Mucocele in 1901.
Classification of surgical approaches used in the management of mucoceles of paranasal sinuses:
I Transnasal approaches: This include Endoscopic sinus surgery, Microscopic sinus surgery, Trans sphenoidal approach.
Etiopathogenesis:
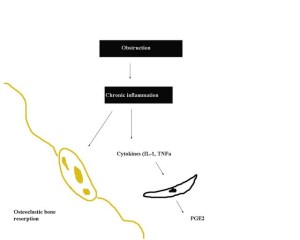
Mucoceles have been postulated to form due to obstruction of sinus ostia following chronic infections / allergic reactions involving paranasal sinuses 3. Previous trauma / surgery can also cause obstruction to sinus outflow channels causing formation of mucoceles. Ethmoiodal mucoceles if present in isolation could be caused by endoscopic ethmoidectomy. Some studies have reportedoccurrence of isolated ethmoidal mucoceles even 10 years after surgery 6. Paranasal sinuses continues to expand slowly owing to pent up mucous secretions. These mucoceles are lined by dilated ciliated columnar epithelium which secrete mucous causing expansion of the cyst. Continuing expansion of this cyst puts pressure on the bony walls of paranasal sinuses, causing bony erosion andremodeling. Unchecked extension of sinus cavity can cause extension of mucocele into orbit, nasopharynx and cranial cavity9. In addition to pressure changes inflammatory mediators like prostaglandins, interleukins and tumor necrosis factor present within mucoceles also contribute to their expansion capability 10.
Three main theories of pathogenesis of mucocele formation has been postulated8:
1. Pressure erosion
2. Cystic degeneration of glandular tissue
3. Active bone resorption and regeneration
Sites involved by mucoceles :7
1. Anterior ethmoid
2. Frontal
3. Maxilla
4. Posterior ethmoid
5. Sphenoid
About 60% of paranasal sinus mucoceles are present in the frontoethmoidal region 11.
Relationship between endoscopic sinus surgery and mucocele formation:
Endoscopic surgery can cause mucocele formation due to adhesions developing in the middle meatus. This complication can be prevented by taking care not to damage normal mucosa. Retention of healthy mucosa in the middle meatal area prevents adhesions from occurring. Meticulous post operative endoscopic cleaning of crusts will help in minimizing adhesion formation. Routine middle turbinate excision while performing endoscopic sinus surgery was previously considered to minimize adhesions from occurring in the middle meatus area. Adhesions can still form in other areas of nasal cavity. In fact adhesions can form between remnant middle turbinate and lateral nasal wall 6. Studies have revealed that it could take anywhere between 5 – 10 years6 before mucocele develops, hence it is important to elicit history of paranasal surgery in these patients.
Clinical features:
Usually patients with mucoceles involving paranasal sinusesdon’thave nasal / sinus symptoms. Only symptoms they present with are ophthalmological in nature.


1. Pain: This is commonly periorbital in nature. This is caused by inflammation and stretching of nasal and sinus mucosa, rarely from dura. Pain is usually transmitted by trigeminal nerve 12.
2. Progressive proptosis
3. Visual disturbances (diplopia) / blurring of vision: This is caused by erosion of the bony casing around optic nerve. Any further expansion of mucocele will cause compression of optic nerve compromising its blood supply. Infections from mucocele can reach the optic nerve when the bony casing around the optic nerve is breached by the enlarging mucocele 14.
4. Epiphora
5. Impaired ocular mobility
Role of radiology in diagnosis of mucoceles:
Radiological images of sinuses demonstrate thinning and expansion of affected paranasal sinus walls. Sinuses affected by mucoceles usually appears homogenous and airless. Plain x-ray of paranasal sinus mucoceles show the following features:
1. Soft tissue density mass seen obliterating sinuses
2. Expansion of paranasal sinus
3. Evidence of bone thinning and erosion
CT scan shows lesions with greater clarity. Precise extension of the lesion can be assessed by studying CT scan images. Scans reveal well defined expansile lesion with obliteration of paranasal sinus air cell cavities.


Size of the swelling (external) caused by frontoethmoidal mucoceles increases in size gradually. The rate of expansion of frontoethmoidal mucocele is accelerated if secondary infection is present within mucocele 13.
Classification of Frontal mucocele:
Frontal mucoceles have been classified into 5 types depending on its extent.
Type I: In this type the mucocele is limited to the frontal sinus only with or without orbital extension.
Type II: Here the mucocele is found involving the frontal and ethmoidal sinuses with or without orbital extension.
Type IIIa: In this type the mucocele erodes the posterior wall of the frontal sinus with minimal or no intracranial involvement.
Type IIIb: In this type the mucocele erodes the posterior wall with major intra cranial extension.
Type IV: In this type the mucocele erodes the anterior wall of the frontal sinus.
Type Va: In this type there is erosion of both anterior and posterior walls of frontal sinus without or minimal intracranial extension.
Type Vb: In this type there is erosion of both anterior and posterior walls of frontal sinus with a major intracranial extension.
Management
Mucoceles are ideally managed surgically. Before the advent of endoscopic procedures, External frontoethmoidectomy was considered to be the ideal management modality.
Classification of surgical approaches:
I. Transnasal approach:
Endoscopic sinus surgery
Microscopic sinus surgery
Trans sphenoidal approach
II. External approaches:
Caldwel Luc approach
Osteoplastic frontal sinus surgery
External Ethmoidectomy
Lateral rhinotomy
Craniofacial resection
Endoscopic procedures are currently the commonly used surgical approach in managing mucoceles.


References
- Canalis RF, Zajtchuk JT, Jenkins HA. Ethmoidal mucoceles. Arch Otolaryngol Head Neck Surg 104:286-291, 1978.
- Natvig K, Larsen TE. Mucoceles of the paranasal sinus. J Laryngol Otol 92: 1075-1 082, 1982.
- Evans C. Aetiology and treatment of fronto-ethmoidal mucocele. J Laryngol Otol 95:361-375,1981.
- Lai PC, Liao SL, Jou JR, et al. Transcaruncular approach for the management of frontoethmoid mucoceles. Br J Ophthalmol 2003;87: 699-703.
- Christmas DA, Mirante JP, Yanagisawa E. Isolated ethmoid sinus mucocele. ENT Rhinoscopic Clinic 2002;759-60.
- Busaba NY, Salman SD. Ethmoid mucocele as a late complication of endoscopic ethmoidectomy. Otolaryngol Head Neck Surg 2003;128: 517-22.
- Sinus mucocele: Natural history and long-term recurrence rate M. Devars du Mayne, A. Moya-Plana, D. Malinvaud, O. Laccourreye, P. Bonfils European Annals of Otorhinolaryngology, Head and Neck diseases (2012)
- https://sites.google.com/site/drtbalusotolaryngology/rhinology/mucocele
- Lai PC, Liao SL, Jou JR, et al. Transcaruncular approach for the management of frontoethmoid mucoceles. Br J Ophthalmol 2003;87: 699-703.
- Conboy PJ, Jones NS. The place of endoscopic sinus surgery in the treatment of paranasal sinus mucoceles. Clin Otolaryngol 2003;28:207-10.
- Har-El G. Endoscopic management of 108 sinus mucoceles. The Laryngoscope. 2001;111:2131---4.
- Moriyama H, Hesaka H, Tachibana T, Honda Y. Mucoceles of ethmoid and sphenoid sinus with visual disturbance. Arch Otolaryngol Head Neck Surg 1992;118:142–6.
- Lai PC, Liao SL, Jou JR, et al. Transcaruncular approach for the management of frontoethmoid mucoceles. Br J Ophthalmol 2003;87: 699-703.
- Yumoto E, Hyodo M, Kawakita S, Aibara R. Effect of sinus surgery on visual disturbance caused by spheno-ethmoid mucoceles. Am J Rhinol 1997;11:337–43.

Leave a comment